Describe the medical necessity provision of the ipf pps. IPF Billing Guide 2022-12-25
Describe the medical necessity provision of the ipf pps Rating:
4,3/10
1838
reviews
The medical necessity provision of the Inpatient Prospective Payment System (IPF PPS) is a critical aspect of the Medicare payment system for inpatient psychiatric facilities (IPFs). This provision specifies the criteria that must be met in order for a patient's stay in an IPF to be considered medically necessary and eligible for reimbursement under Medicare.
The medical necessity provision is based on the principle that Medicare will only cover services that are medically necessary and reasonable for the treatment of a patient's condition. In order to meet this requirement, the IPF PPS requires that a patient's stay in an IPF must be deemed necessary by a physician and be supported by documentation of the patient's clinical condition.
The medical necessity provision also requires that a patient's stay in an IPF be limited to the shortest duration necessary to achieve the goals of treatment. This means that the IPF must continually assess the patient's progress and determine whether continued treatment is necessary, or whether the patient is ready to be discharged.
In addition to these requirements, the medical necessity provision also includes specific criteria for the type of treatment that can be provided in an IPF. For example, the IPF must provide a range of therapeutic interventions, such as individual, group, and family therapy, as well as medications and other medical treatments, as needed.
Overall, the medical necessity provision of the IPF PPS is an important aspect of the Medicare payment system that ensures that patients receive the necessary level of care while also ensuring that taxpayer funds are used wisely. It helps to ensure that patients receive the best possible treatment for their conditions and that IPFs are held to high standards of care.
Medical Necessity: Why It Matters, Ways to Demonstrate It
Alaska ranges from 1. Is the principal diagnosis complicated? Patient X was admitted to Happy Hospital and had an admission with a LOS of 8 days. Each comorbidity grouping will receive a grouping-specific adjustment. For ages 65-69, the adjustment factor is 1. A variable per diem adjustment factor depends on several things.
If 75% of the 60-day period was completed, then 75% of the reimbursement rate is paid. In Alaska and Hawaii, there are varying cost of living adjustment factors. Facilities with CCRs outside of trim points use national rural urban CCRs. An adjustment was implemented for older patients because regression analysis shows the cost per day as increasing with increasing patient age. Payment rates are to be established in advance and fixed for the fiscal period to which they apply Payments rates are not automatically determined by the hospital's past or current actual cost Prospective payment rates are considered to be payment in full The hospital retains the profit or suffers a loss resulting from the difference between the payment rate and the hospital's cost, creating an incentive for cost control The discharge position identifies where the patient goes for care after discharge. The three-digit code F02 Dementia in other diseases classified elsewhere is designated a Code First diagnosis, indicating that all diagnosis codes that fall under the F02 category codes F02.
Functional integration is the integration, across all units in the IDS, of the functions that support the delivery of direct patient care, such as financial management, information systems, human resources, and other support services. The Medicare Claims Processing Manual, chapter 3 — Inpatient Hospital Billing, section 190. Part of our responsibility as healthcare business professionals is to understand the financial realities of healthcare delivery and reimbursement. Written policies and procedures are rules by which the facility and its employees go by while working. If the discharge disposition indicates that the patient is to receive post-acute care i. You should ensure all active medical treatment and diagnoses are captured in the medical record documentation, and remind practitioners to connect clinical dots to substantiate treatment patients receive.
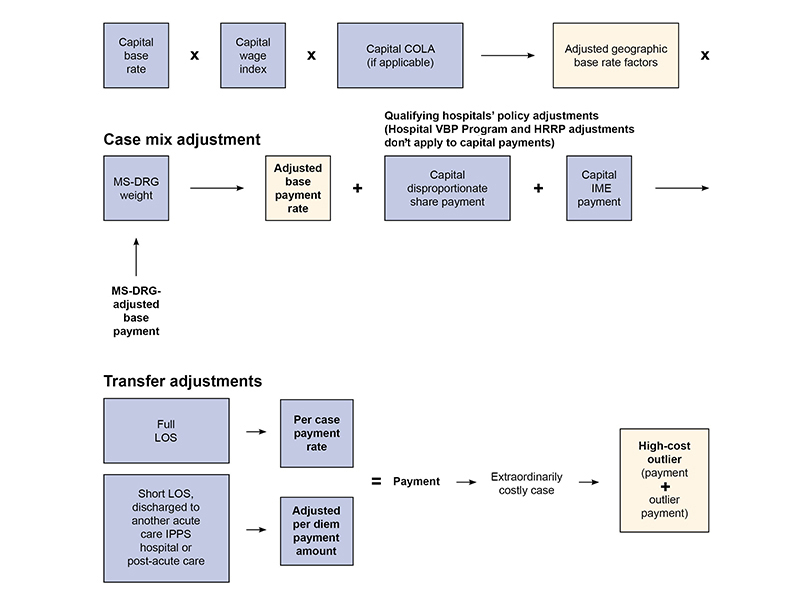
MS-DRG 901 has a GMLOS of 9 days and the relative weight of 4. Outlier — An additional payment made by Medicare for high-dollar claims, intended to protect hospitals from large financial losses due to unusually expensive cases. For example, DRG 885 receives an adjustment factor of 1. Formulating Base and Adjustment Rates Each year, the base rate is set and then adjusted using several factors to formulate the calculated base rate for an individual facility. MS-DRG group assignment: claim sent to MAC, if found clean by grouper MS-DRG assigned based on demographics and coded data, then base rate adjusted for geographic factors times the MS-DRG relative weight.
The Ins and Outs of Inpatient Psychiatric Facility Perspective Payment System
The IPFs affected by the PPS are freestanding psychiatric facilities, distinct part psychiatric units of acute care hospitals, and distinct part units of critical access hospitals Several factors may adjust the payment: The federal wage index adjustment, which is applied to the labor portion of the service, an add-on of 17 percent for facilities in rural areas, and an adjustment made for qualified teaching facilities of 0. Initial stay provision: Higher payment is provided for initial days of stay to compensate for the higher costs associated with new admissions. This is different from the Medicare hospital inpatient prospective payment system, where a complication or comorbidity CC or major complication or comorbidity MCC would change the DRG, thus changing the payment; rather, comorbid conditions that fall into a comorbidity category add another adjustment factor. Medicaid Definition of "Medically Necessary" There isn't a definitive interpretation for "medically necessary" for the federally mandated, state-administered Although there are differences in each state, they often correspond to the Medicare definition of prescriptions and services "necessary for diagnosis or treatment of the condition, illness, or injury. If a patient is discharged and then readmitted within two days, the two admissions count as one admission. Identify how injuries occur.
Readmission provision: Because facilities have a higher adjustment at the beginning of the admission, the Centers for Medicare and Medicaid Services CMS implemented the readmission provision to prevent premature discharge and then remittance of patients. Table A Name of Specific DRG DRG Adjust Degenerative nervous system disorders with MCC 056 1. She is a member of the Florence, Ky. Education training helps those newly hired or who need refresher courses in job skills to be able to be properly trained. The x-ray provides a definitive diagnosis, while an additional chest MRI or a lung biopsy may be considered "medically necessary" for treatment.
Principals of Health Reimbursement CHAPTER 6 Flashcards
The adjustments recognize the higher cost incurred in the early days of a stay. Get a Lawyer The information surrounding what constitutes a medically necessary procedure or course of treatment is confusing and complex. She has approximately 20 years of experience in a variety of health information management roles. Government experts then analyze and use the comments to make any necessary changes before the proposed rule is published as a final rule in the Federal Register. The term "medically necessary" is important because it helps to determine what Medicare, Medicaid, and private insurance companies will pay for. The physician of record must connect any conditions the patient may have with the treatment during the encounter.
Electroconvulsive Therapy: It is costly and twice as expensive than others. The Length-of-Stay Adjustment established as a result of data showing that per diem costs for psychiatric cases decrease as LOS increases Comorbid Condition Adjustment used because 2002 data showed that there is a need to provide payment adjustment for certain comorbidities, such as developmental disabilities or uncontrolled diabetes mellitus. Receiving hospital bills claim as usual. Stop-loss provision: Was used as the phase-in period for this prospective payment system PPS. According to the 2015 IPF PPS final rule, comorbid conditions must exist at the time of admission or develop subsequently, and must affect the treatment received, length of stay, or both.
The adjustments were derived using regression analysis to determine relevant factors to predict patient resources. A child who has end-stage renal disease Process integration, also known as clinical integration, is the coordination of direct patient care activities. An intermediary is usually, but necessarily, an insurance company, such as Blue Cross. Inlier — A time covered by the Medicare Severity-Diagnosis Related Group MS-DRG payment period of a claim that includes fully paid days, coinsurance days, or days after benefits have exhausted. MedPAC provides an annual assessment of all Medicare prospective payment systems with recommendations to Congress. The adjustment amount is based on the percentage of days in the episode of care that were completed. Code symptoms, if no definitive diagnosis is yet determined, instead of using rule-out statements.
If a qualifying OR was NOT performed, the case is assigned medical status. The cost is mostly associated with the increased length of stay and also as a result of increased of ancillary services. The facility can receive a single comorbidity adjustment per comorbidity category; however, it can also receive an adjustment for more than one comorbidity category per encounter. Additional payments are provided for cost outlier cases, and qualifying emergency department ED electroconvulsive therapy ECT treatments. If your medical claim was denied due to the lack of medical necessity, you have the right to appeal the insurer's decision.