Skeletal malocclusion. Managing Skeletal Problems in Pediatric Malocclusion 2023-01-01
Skeletal malocclusion Rating:
8,6/10
1631
reviews
The "Ballad of Birmingham" is a poem written by Dudley Randall in the 1960s. It tells the story of a young girl who wants to participate in a civil rights demonstration in Birmingham, Alabama, but her mother objects, fearing for her safety. The girl persists, saying that she wants to march for freedom and justice like the civil rights leader, Martin Luther King Jr. Ultimately, the mother relents, and the girl is able to attend the demonstration.
The poem is a poignant reflection on the Civil Rights Movement, and the sacrifices and dangers faced by those who fought for justice and equality. The central theme of the poem is the struggle for civil rights and the determination of individuals to stand up for what they believe in, even in the face of adversity and danger.
The poem is set in the context of the Civil Rights Movement, which was a time of great tension and conflict in the United States. During this time, African Americans were fighting for their rights and for equal treatment under the law. The "Ballad of Birmingham" reflects this struggle, as the young girl in the poem wants to participate in a civil rights demonstration and stand up for what she believes in.
The mother in the poem represents the fears and concerns of many African Americans during this time. She is worried about the safety of her child and doesn't want her to get involved in the civil rights movement. However, the girl is determined to stand up for what she believes in, and her mother ultimately agrees to let her go to the demonstration.
The "Ballad of Birmingham" is a powerful and moving poem that speaks to the struggles and sacrifices of the Civil Rights Movement. It is a poignant reminder of the importance of standing up for what we believe in and fighting for justice and equality.
Skeletal Malocclusion Treatment
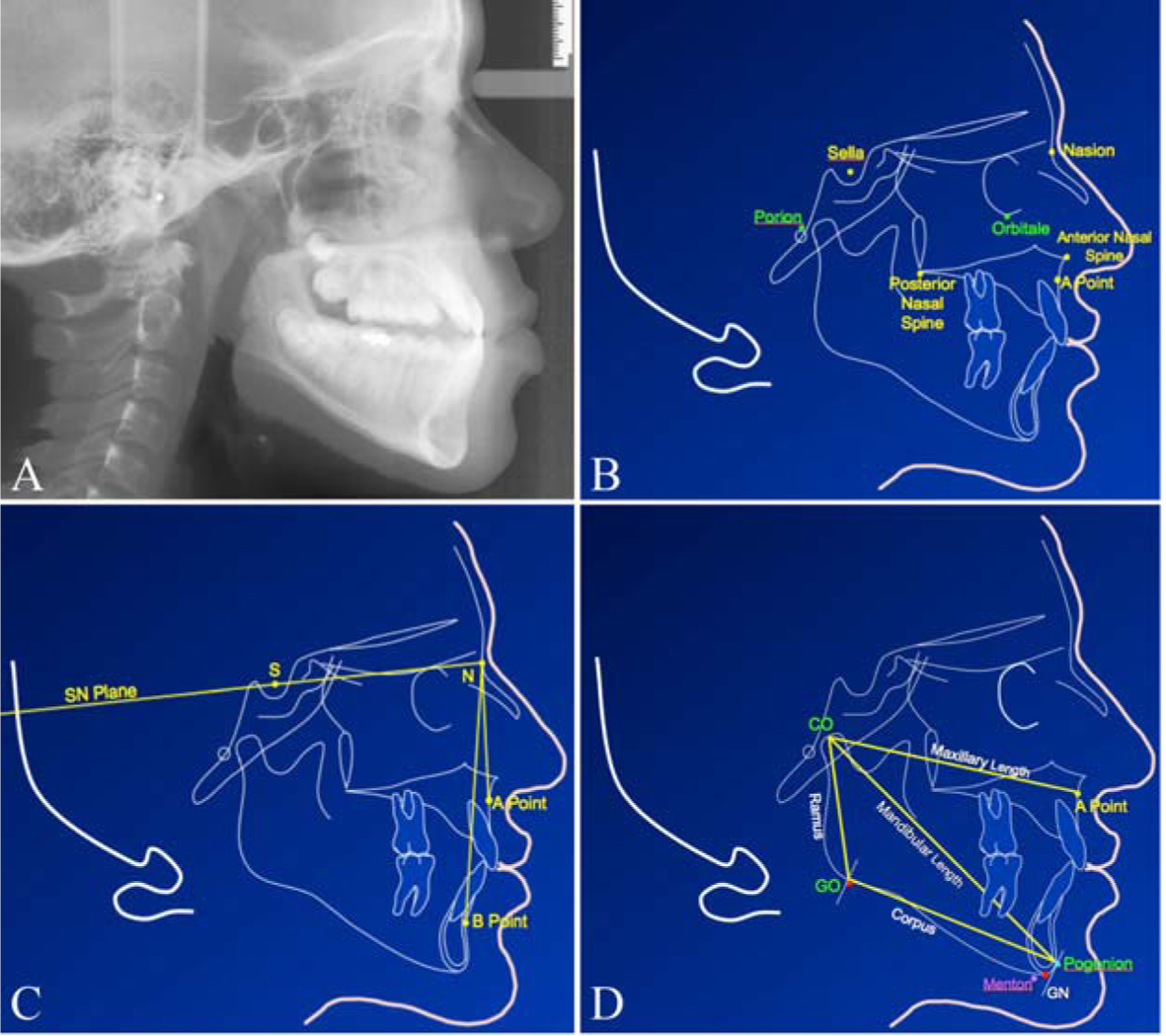
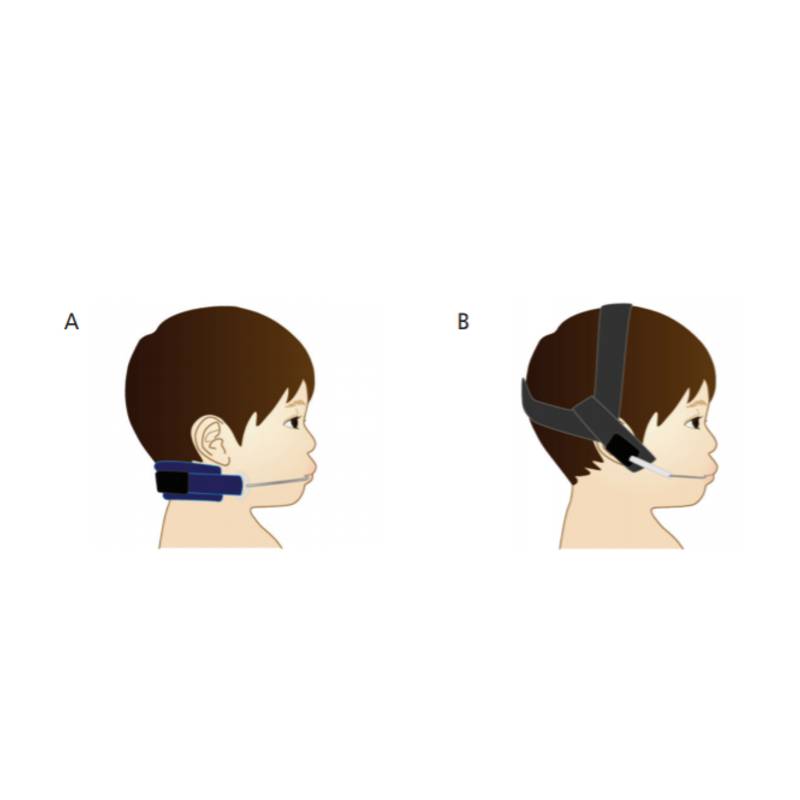
Real class III jaw deformity, which is mostly caused by malposition of the lower jaw, upper jaw, or both, often require more complex treatments. Digital or traditional bite impressions and X-rays are taken to determine the best treatment program before prescribing correctional appliances. Am J Ortho Dentofac Orthop. Chincup treatment modifies the mandibular shape in children with prognathism. Several systematic reviews conclude FAs can reduce overjet, correct molar relationships, and reduce the severity of Class II malocclusion. By choosing the skeletal surgery alternative, she was able to eliminate all of the surgeries and get the facial support and missing teeth replaced much quicker.
Identifying and Treating Malocclusions Classes I, II, and III
MANAGING SKELETAL CLASS II MALOCCLUSION In a growing patient, the best way to correct Class II malocclusion is through growth modification. If the class III jaw deformities was because of mandibular excess, it most probably would require surgery. Am J Orthod Dentofacial Orthop. The maxillofacial skeleton in growing children is adaptable to change from both internal and external forces. In Class II cases without PTID, mandibular retrusion is due to a true micrognathic mandible, and early expansion can enhance forward growth of the mandible. Depending on the type and severity of the malocclusion, health problems can result, including sleep apnea and gum disease. J World Fed Orthod.
Managing Skeletal Problems in Pediatric Malocclusion
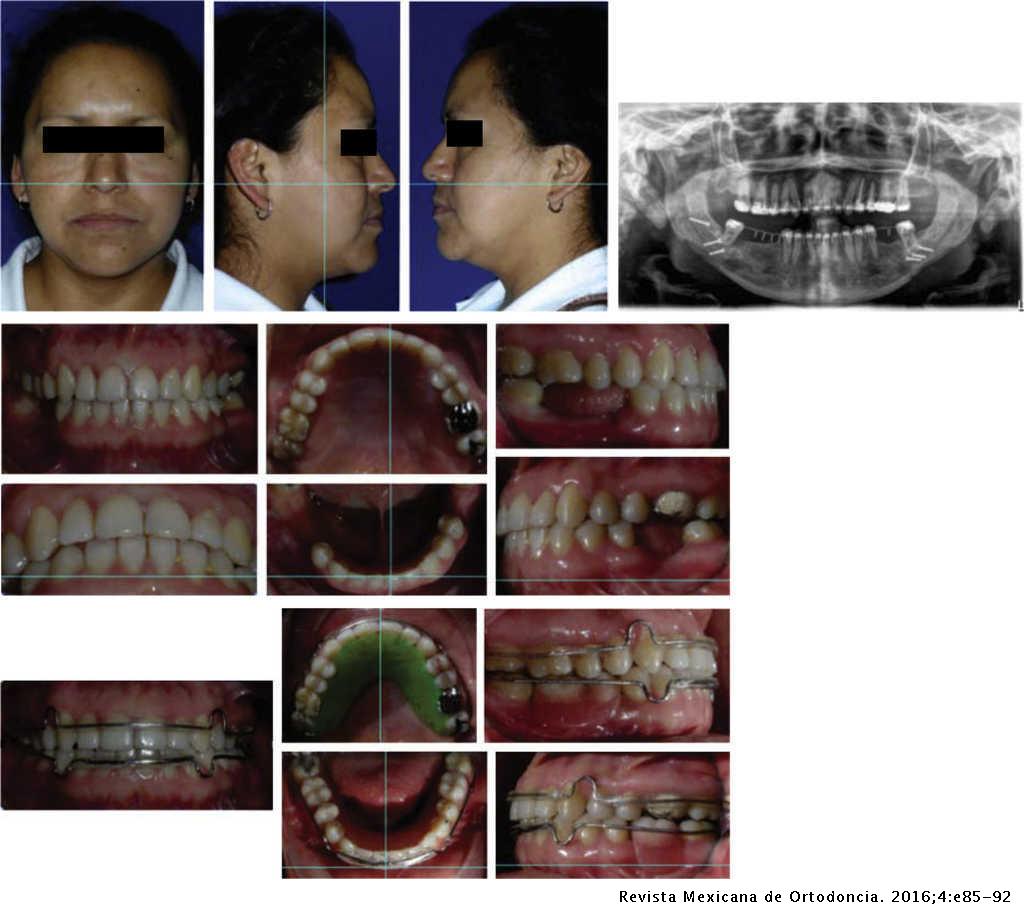
Jamilian, an orthodontist, has a specialized fellowship in orthodontic surgery and maxillofacial abnormalities and is a full-time professor in the orthodontics department of the Dentistry School of the Islamic Azad University. The linguoverted canine is then often in traumatic contact with the roof of the mouth. The answer is no because the patient has spaces between her teeth that porcelain veneers cannot close. One-third of the United States population aged 6 to 17 have Class II occlusion. A randomized controlled study of early headgear treatment on occlusal stability — a 13 year follow-up. What are some common forms of dental malocclusion? Find treatment options specific to each Associated Problems Crowding Spacing Bimaxillary dentoalveolar protrusion Posterior crossbites.
Class II occlusion cannot self-correct and, in some cases, can worsen with age. Hengsheng Lin, BDS, MSD, is a clinical professor in the Department of Orofacial Sciences at the University of California, San Francisco School of Dentistry. This is the most common kind of malocclusion. Common treatment uses headgear to restrain the maxillary forward growth if there is excess maxillary growth, or a functional appliance to advance the mandible if there is a retrusive lower jaw. When the bite is closing, and if the mandible is guided by an early intermaxillary abnormal contact, the mandible can either move laterally or in a forwards direction.
In the first type, which is called functional or pseudo class 3, the If diagnosed and treated early, this problem could be resolved by orthodontic treatments and without any need for surgery. Treatment response and long-term dento-facial adaptations to maxillary expansion and protraction. Aside from clinical dentistry, she also consults for several different organizations, including Dr. MANAGEMENT OF ANTERIOR CROSSBITE AND CLASS III MALOCCLUSION Class III malocclusion can range from a simple anterior crossbite to severe skeletal discrepancy. Occlusion is a term used to describe the way teeth align with each other. FIGURES 4A through 4C. Excessive use of pacifiers, thumb sucking, or tongue thrusting in children from one to three years old may force baby teeth and, eventually, permanent teeth to erupt in overbite positions.
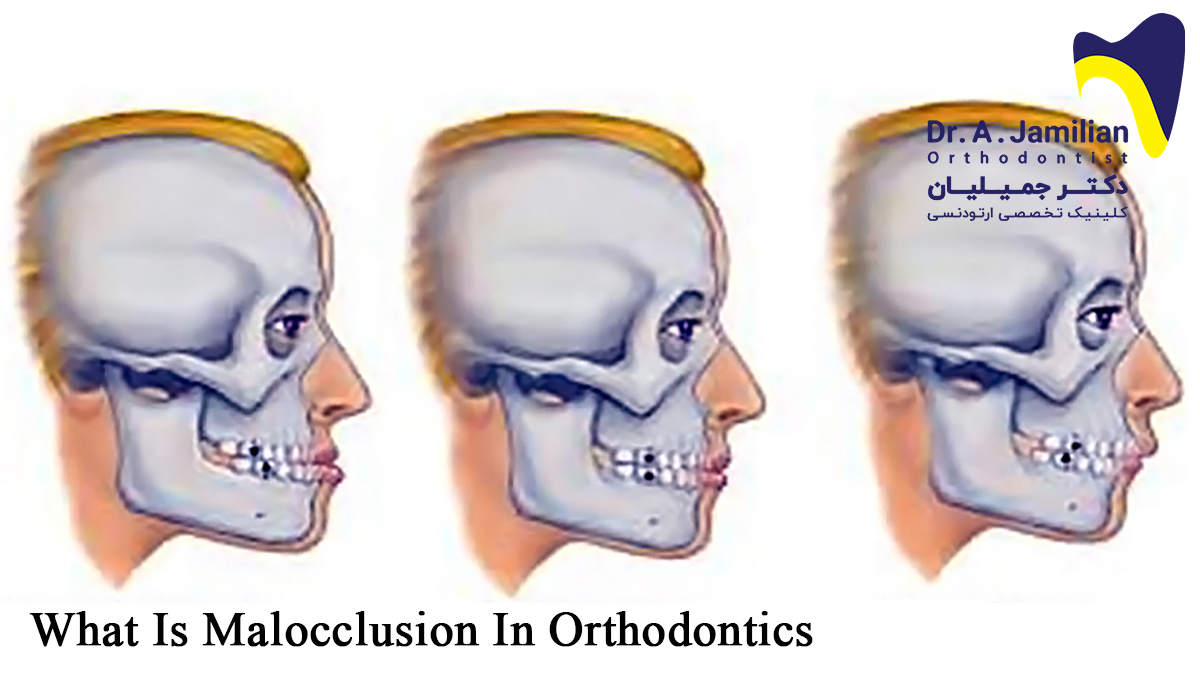
What are some common forms of skeletal malocclusion? In severe Class II cases, these appliances can be combined. This is commonly called an underbite. It has a significant influence on the facial appearance, speaking abilities, ease of chewing and dental malocclusion. An orthopedic approach to the treatment of Class III malocclusion in young patients. The asymmetry may occur in a number of different ways.
8 The aetiology of malocclusion: (i) skeletal and soft tissue factors
Overbites occur when Causes of Malocclusions Malocclusions can occur in baby teeth or permanent teeth. C The interaction between the anteroposterior and transverse dimension. Furthermore, in sagittal, vertical and transversal discrepancies, skeletal deviations can be involved, combining both dental and skeletal discrepancies. The short-term treatment effects of face mask therapy in Class III patients based on the anchorage device: miniplates vs rapid maxillary expansion. The upper incisors are retroclined, and lower incisors may be proclined and show tissue damage. Displacement and stress distribution of the maxillofacial complex during maxillary protraction with buccal versus palatal plates: finite element analysis.
Finally, there may be an asymmetry that is exhibited as an abnormal increased space between the upper and lower jaws may affect one or both sides and is referred to as an open bite. Sample treatment of a 5-year-old: Use upper sliding lingual arch to correct anterior crossbite in five months A through C. An estimate of craniofacial growth in Class III malocclusion. Malocclusion refers to abnormal tooth alignment. A systematic review and meta-analysis showed that compared to a control group, patients using headgear had a resulting change of -1.
. This may have contributed to the development of the increased curve of Spee in the upper arch and the anterior open bite. Therefore, treatment could be carried out in developmental stages if required and complex treatments in later stages will be avoided. Assessment of treatment requirement is based on an evaluation of the risk, short or long term, for disturbances in oral health, function, aesthetics or patient satisfaction. The most important reason to initiate early orthodontic treatment in children is to correct or reduce the severity of malocclusion and skeletal discrepancy, and allow normal maxillofacial growth and development.