Clagett procedure of chest wall. The Use of Human Acellular Dermal Matrix for Chest Wall Reconstruction 2022-12-13
Clagett procedure of chest wall Rating:
5,7/10
1942
reviews
The Clagett procedure is a surgical procedure that is used to repair chest wall deformities, such as pectus excavatum (sunken chest) or pectus carinatum (pigeon chest). It is a complex procedure that involves the removal of excess bone and cartilage from the rib cage, as well as the placement of internal braces or struts to help support and reshape the chest wall.
The Clagett procedure was first described by Dr. John Clagett in the 1960s, and has since become a well-established technique for correcting chest wall deformities. It is typically performed on adolescents or young adults, as the chest wall is still growing and more responsive to surgical correction at this age.
The surgery is typically performed under general anesthesia and takes several hours to complete. During the procedure, the surgeon makes an incision in the chest and removes excess bone and cartilage from the rib cage to help reshape the chest wall. They may also insert internal braces or struts to help support and stabilize the chest wall as it heals.
After the surgery, patients will typically need to stay in the hospital for several days to recover. They will also need to follow a specific post-operative care plan, which may include physical therapy and medications to manage pain and swelling.
The Clagett procedure is generally considered safe and effective, with a high success rate in correcting chest wall deformities. However, as with any surgery, there are risks involved, including the risk of infection, bleeding, and complications from the anesthesia.
In conclusion, the Clagett procedure is a complex surgical procedure used to repair chest wall deformities such as pectus excavatum or pectus carinatum. It involves the removal of excess bone and cartilage and the insertion of internal braces or struts to help reshape and support the chest wall. While it is generally considered safe and effective, there are risks involved as with any surgery.
Care of the patient with Clagett open
Do you think it is important that it is distributed all over the thoracic cavity? Analgesic administration should be coordinated with respiratory care and movement. After day 8 of pleural space irrigation, 20 patients had negative Gram stains. One would predict that the results would be excellent, but 100% is indeed outstanding. These products are cleared for use in a variety of soft tissue augmentation procedures including dural repair, chest wall reconstruction, cardiac and cardiovascular surgery, abdominal wall repair, and pelvic organ prolapse repair. Furthermore, the treatment protocols have not accounted for a potential difference in the pathophysiology of early versus late PNE. J Thorac Cardiovasc Surg.
Understanding Procedural Coding Chapter 7 Respiratory System Flashcards
Fluid is cultured and the appropriate antibiotics are given Alexander ; Fetter, 1992. We respectively reviewed all patients who underwent chest wall reconstruction with a biosynthetic material from January 2020 to June 2021. This cycle was continued until a negative Gram stain was obtained. Synthetic materials have been the mainstay for reconstruction. After prevention, a high index of suspicion and an aggressive approach to the diagnosis play a significant role in decreasing the morbidity and mortality of PNE. These scenarios must be anticipated before surgery to optimize preoperative preparation, minimize postoperative morbidity and mortality, and improve oncologic outcomes. The nurse must assess the patient for complications such as pneumonia, sepsis, respiratory failure, and cardiac insufficiency.
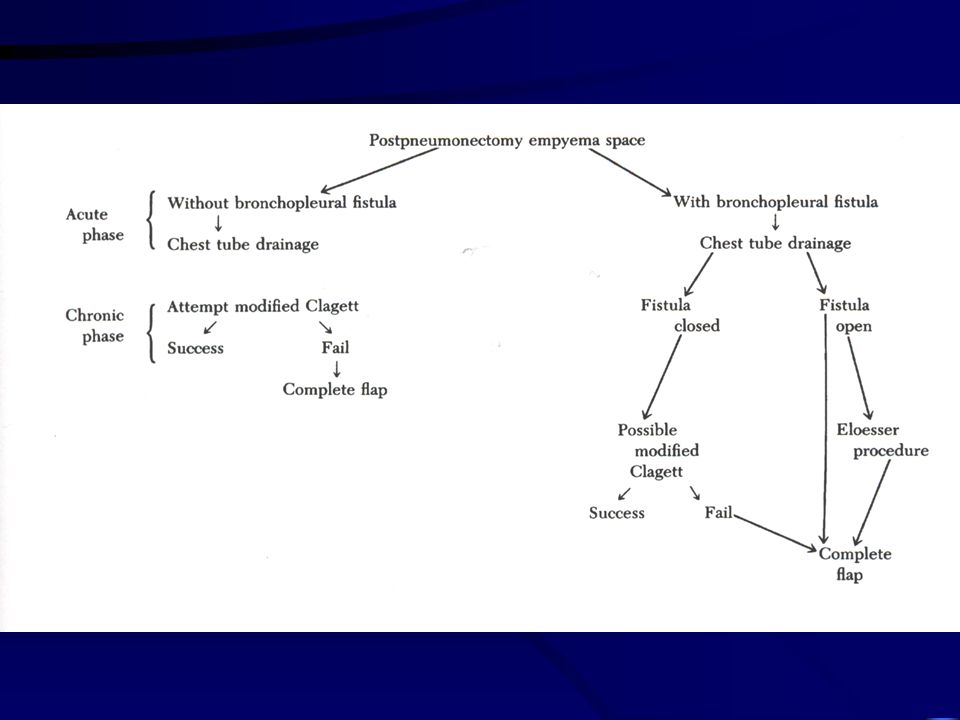
The physician usually does the first dressing change. The incidence of empyema following a pneumonectomy is 13%, whereas the incidence is estimated to be between 1% and 4% following other pulmonary resections Alexander a Fetter, 1992. In patients with predisposing risk factors, the bronchial stump should be reinforced with vascularized tissue in the form of the omentum, pericardial fat pad pedicle, or chest wall muscle. A pneumonectomy is usually done when metastasis has occurred to the lobar and hilar lymph nodes or when a lobectomy will not remove the entire tumor. Active infection in the form of resection in the face of inflammatory conditions, bronchiectasis, presence of postobstructive pneumonitis, gross contamination of the pleural space, and sputum cultures positive for tuberculosis increases the risk of PNE.
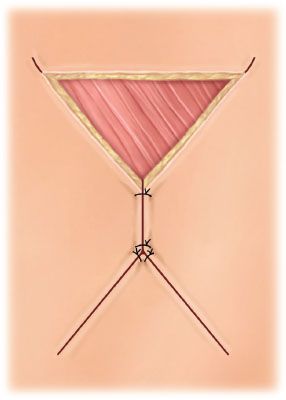
Closure of chest wall following open flap drainage for empyema Clagett type
The patient may be malnourished and in a catabolic state due to the extent and duration of infection and history of lung cancer with associated radiation or chemotherapy treatment. Our aim is to highlight these clinically challenging anatomic presentations that can be encountered in patients with retroperitoneal sarcomas. The patient should be turned only to the operative side to prevent leakage of fluid to the good lung. The 2-stage procedure consisted of open pleural drainage, closure of the BPF, removal of the necrotic tissue, and secondary closure or obliteration of the pleural cavity with antibiotic solution. .
D quit smoking I year ago. Three patients in our series had undergone preoperative radiotherapy. Esophageal diversion is often required when extensive tissue loss precludes primary repair. Postoperative complications occurred in 6 patients 24%. The Clagett procedure was less mutilating, more successful, and had a lower morbidity and mortality than thoracoplasty Shamji et al.
The Use of Human Acellular Dermal Matrix for Chest Wall Reconstruction
D are adjusting well and are excited about the progress that has been made thus far. The patients were diagnosed with tracheal adenoid cystic carcinoma by histopathological biopsy. The large open-window thoracostomy may be permanently left open or covered with skin grafts. The perfect material does not exist to restore chest wall stability. Reconstruction was performed with a combination of bovine pericardium and PLA bars in 11 patients 44% , bovine pericardium alone in 10, and PLA bars alone in 4; muscle flaps were interposed in 7 patients 28%. All patients had a bronchopleural fistula. In contrast, if the bronchus has dehisced at the level of the carina, a complete suture reclosure may be impossible without some type of tissue reinforcement.
Pleural space irrigation and modified clagett procedure for the treatment of early postpneumonectomy empyema
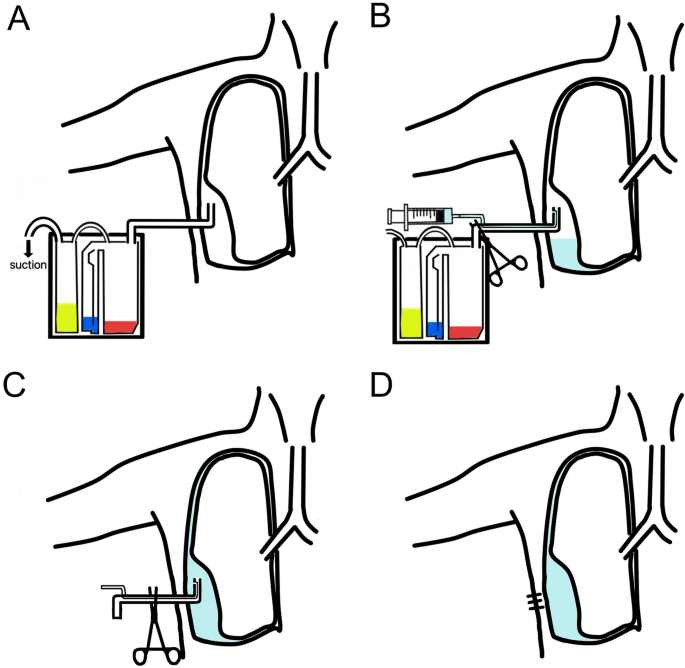
The skin was closed with interrupted mattress sutures of 3-0 nylon, and deep retention mattress sutures of 1-0 nylon were placed intermittently to decrease the tension on the skin closure. D could return to work. During the second stage, when the pleural space was clean and sterile, the space was filled with 0. The pleural space was irrigated with 0. PathophysiologyFollowing a pneumonectomy, there is air in the pleural cavity The air is gradually absorbed and the space fills with serous and serosanguinous fluid.
Comparison of continuous epidural block and continuous paravertebral block in postoperative analgaesia after video-assisted thoracoscopic surgery lobectomy: a randomised, non-inferiority trial. In the authors' collective review, the fistulas were small, the empyemas early, and the cavities obliterated with antibiotic solution. ANOVA and Tukey's post hoc test demonstrated the highest mean γ wof int value 90. The original surgeon then referred the patient to another physician and facility for further treatment. This modification of the Clagett procedure requires 1 surgical procedure and results in significantly shorter hospitalization and decreased morbidity in this selected subset of patients with PNE. The empyema that develops prevents successful closure of the bronchopleural fistula Duhaylongsod ; Wolfe, 1992. We have assessed the patient multidisciplinary with cardiovascular and plastic reconstructive esthetic surgery for non-healing scar.
To assist the patient and family, the nurse should provide reassurance and emotional support by allowing the patient and family to verbalize feelings and frustrations. Two patients with bronchiectasis had completion pneumonectomy. One catheter was placed overlying the mediastinum, and the other was placed onto the posterolateral chest wall. Although this approach has been successful in up to 92% of cases, it results in prolonged hospitalization, repeated operative procedures, and significant morbidity. Simple drainage and irrigation in this chronic situation simply does not work. The mean hospitalization time was 12.